Case of 65 years old with pain in right lower limb, fever, Shortness of breath
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
Case of 65years old with Pain in right lower limb, fever and shortness of breath since 1 week.
CHIEF COMPLAINT:
HISTORY OF PRESENT ILLNESS:
PAST HISTORY:
TREATMENT HISTORY:
PERSONAL HISTORY:
1.Diet-mixed
2.Appetite: decreased since 1 week
3.Bladder movements - decreased since 1 year
4.Bowel: constipation, passes stools for every 2-3 days
5. Sleep -adequate
6.Addictions-nil
FAMILY HISTORY:
GENERAL EXAMINATION:
The patient was examined in a well-lit room after informed consent was taken.
She is conscious, coherent, cooperative, well oriented to time, place and person, well nourished and moderately built.
No pallor, Icterus, Clubbing, Cyanosis, Koilonychia, Lymphadenopathy, Edema.




VITALS:
- Temp: 99.1 F
- BP: 120/70mm Hg
- PR: 78bpm
- RR: 18cpm
- Spo2: 96% on RA
- GRBS : 87mg/dl
SYSTEMIC EXAMINATION:
INVESTIGATIONS:
TLC: 14100 cells/ cumm
RBC: 4.78 million/cumm
PLT: 4.50 lakh/cumm
PCV: 39.6 vol%
Neutrophils:71 %
Lymphocytes:21 %
Eosinophils: 2%
Monocytes: 6%
MCV: 82.8 fl
MCH:26.6 pg
Peripheral Smear: Normocytic normochromic blood picture with leucocytosis
RFT:
Blood urea: 37 mg/dl
Serum creatinine: 0.8 mg/dl
Serum electrolytes:
Na+: 142 mEq/l
K+: 4.5 mEq/l
Chloride : 99 mEq/l
LFT:
Total bilurubin:0.68mg/dl
Direct bilurubin :0.20 mg/dl
AST:33 IU/L
ALT:43 IU/L
Alk phosphatase:249 IU/L
Total Protien:6.4 gm/dl
Albumin:3.0 gm/dl
A/G ratio: 0.89
CUE:
Albumin:nil
Sugars:nil
Pus cells:2-3/HPF
Epithelial cells:2-3/HPF
RBS: 76mg/dl
Serology: NEGATIVE
USG ABDOMEN AND PELVIS: Impression
1. Right grade I RPD changes.
2. Raised echogenicity of left kidney
USG CHEST: Impression
B/L mild pleural effusion
2D ECHO:
Trivial TR+, No MR/AR
No RWMA, No AS/MS, Sclerotic AV
Good IV systolic function
Diastolic dysfunction +, No PAH/PE.
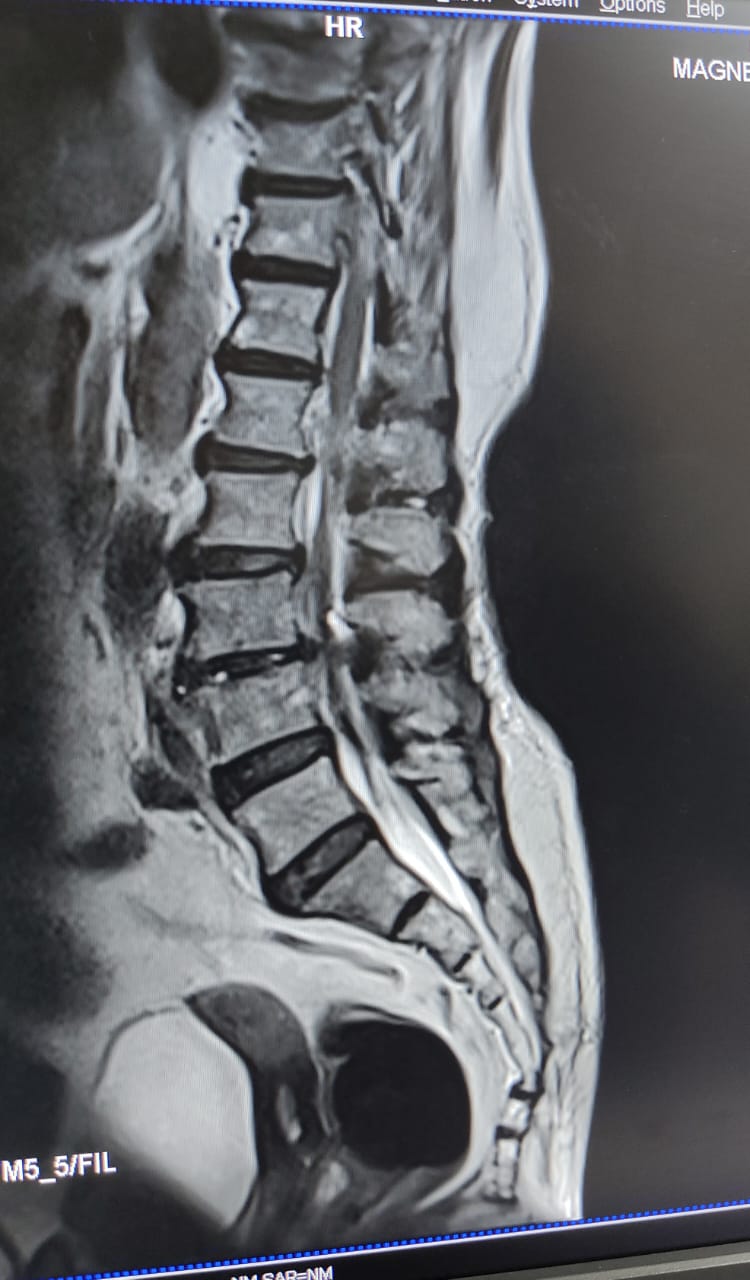
Chest X-ray:

Xray LS spine:decreased L5 disc space.






Comments
Post a Comment